Ureterosigmoidostomy
Ureterosigmoidostomy
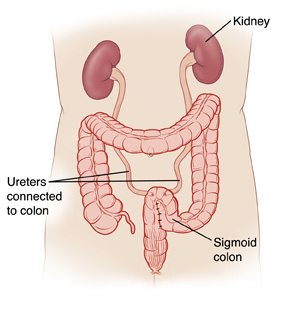
Ureterosigmoidostomy is surgery that creates a new way for urine to pass out of the body. This may be needed if the bladder has been removed due to problems such as bladder cancer. During the surgery, the tubes (called ureters) that carry urine from the kidneys to the bladder are detached from the bladder. They are then attached to part of the colon. This allows both urine and stool to flow through the colon and leave the body through the anus.
Preparing for surgery
Prepare for the surgery as you’ve been told. In addition:
Tell your doctor about all medicines you take. This includes prescription medicines and over-the-counter medicines, vitamins, herbs, and other supplements. It also includes any blood thinners, such as warfarin, clopidogrel, or daily aspirin. You may need to stop taking some or all of them before surgery.
Follow any directions you are given for not eating or drinking before surgery. This includes coffee, water, gum, and mints. (If you have been instructed to take medicines, take them with a small sip of water.)
If you have been told to, prepare your bowel for surgery (called bowel prep). This process begins 1 to 2 days before the surgery. Your doctor may tell you to limit your diet to clear liquids. You may also be asked to take laxatives or to give yourself an enema. Follow all instructions you are given.
The day of surgery
The surgery takes about 3 to 4 hours. Afterward, you will stay in the hospital for 1 to 3 nights.
Before the surgery begins:
An IV (intravenous) line is placed in a vein in your arm or hand. This supplies fluids and medicines (such as antibiotics).
You may receive medicine to prevent blood clots.
To keep you free of pain during the surgery, you’re given general anesthesia. This medicine puts you in a deep sleeplike state through the surgery. A tube may be inserted into your throat to help you breathe.
You may have an epidural to help control postsurgery pain. A small tube is inserted into your back to deliver pain medicine that numbs the lower body. Talk to your doctor or anesthesiologist about this option.
During the surgery:
A cut (incision) is made in the lower belly (abdomen). This is usually from the bellybutton to the pubic bone.
Incisions are made in part of the lower colon. The colon is folded into a U shape and the edges are stitched together with stitches (sutures). This makes a pouch large enough to hold both urine and stool.
A small hole is cut into this part of the colon. A ureter is inserted into the hole. It is then secured to the colon with stitches.
A thin tube (stent) may be placed in the ureter as it heals. The stent helps widen the ureter so urine can flow through it properly.
The same procedure is done on a nearby part of the colon with the second ureter.
When the surgery is complete, the incisions are closed with stitches, staples, or surgical glue.
A tube is put into the rectum to carry urine and stool from the body until healing is complete.
Recovering in the hospital
After the surgery, you will be taken to a recovery room. Here, you’ll wake up from the anesthesia. You may feel sleepy and nauseated. If a breathing tube was used, your throat may be sore at first. When you are ready, you will be taken to your hospital room. While in the hospital:
You will be given medicine to manage pain. Let your providers know if your pain is not controlled.
You’ll first receive IV fluids. In a day or so, you’ll start on a liquid diet. You’ll then slowly return to a normal diet.
As soon as you’re able, you’ll get up and walk.
You’ll be taught coughing and breathing methods to help keep your lungs clear and prevent pneumonia.
The stents in your ureters and the tube in your rectum will likely be removed while you’re in the hospital. If not, you’ll be shown how to care for them at home.
Recovering at home
After your hospital stay, you will be released to an adult family member or friend. Have someone stay with you for the next few days, to help care for you. Recovery time varies for each person. Your doctor will tell you when you can return to your normal routine. Until then, follow the instructions you have been given. Make sure to:
Take all medicines as directed.
Care for incisions as instructed. If you went home with stents or tubes in place, take care of these as you were shown.
Follow your doctor’s guidelines for showering. Don't swim, take a bath, use a hot tub, or do other activities that cause the incision to be covered with water until the doctor says it’s OK.
Not do any heavy lifting or strenuous activities as directed.
Not drive until your doctor says it’s OK. Don’t drive if you’re taking medicines that make you drowsy or sleepy.
Walk a few times each day. Increase your pace and distance as you feel able.
Not strain to pass stool. If needed, take stool softeners as directed by your doctor.
Drink plenty of water. This helps prevent urine odor and dehydration. And follow any other diet instructions you’re given.
When to call your healthcare provider
Call your healthcare provider right away if you have any of the following:
Fever of 100.4°F (38°C) or higher, or as directed by your healthcare provider
Symptoms of infection at an incision site, such as increased redness or swelling, warmth, worsening pain, or foul-smelling drainage
Lower back pain
Problems passing urine or stool
A lot of blood in stool and urine (some blood is normal)
Pain that can’t be controlled with medicines
Nausea or vomiting that won’t go away
Pain or swelling in your legs
Call 911
Call 911 if you have chest pain or trouble breathing.
Follow-up care
You’ll have follow-up visits so your doctor can check how well you’re healing. Stitches, staples, stents, and tubes will be removed as needed. You and your doctor can discuss any further treatment you may need.
Risks and possible complications
Bleeding (you may need a transfusion)
Infection
Blood clots
Greater risk for colon cancer
Urine leakage at the site of the bowel incisions
Abnormal levels of minerals in the blood (you may need lifelong medicine)
Urine backing up into the kidneys
Development of stones in the kidneys or ureters
Damage to the kidneys, ureters, or other nearby organs
Problems passing urine, stool, or both
Risks of anesthesia. The anesthesiologist will discuss these with you.
Updated:
September 02, 2017
Sources:
Atta, MA, Clinical evaluation of patients treated with a detubularised isolated ureterosigmoidosctomy diversion after radical cystectomy, Arab Journal of Urology (2014); 12; pp. 192-196
Reviewed By:
Adler, Liora C., MD,Hanrahan, John, MD,Image reviewed by StayWell medical illustration team.