When Your Child Has a Ventricular Septal Defect (VSD)
When Your Child Has a Ventricular Septal Defect (VSD)
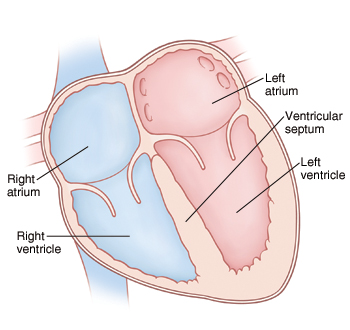
The heart has 4 chambers. A ventricular septal defect (VSD) is a hole in the dividing wall (ventricular septum) between the 2 lower chambers (ventricles) of the heart. A VSD can occur anywhere in the ventricular septum. Left untreated, this defect can lead to certain heart problems over time. But good treatments are usually available.
|
|
Normal heart |
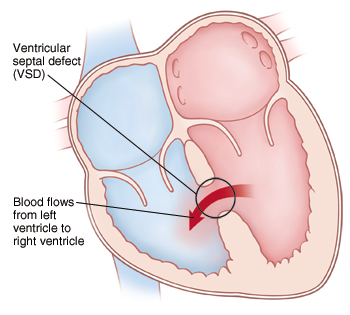
A VSD causes blood to flow from the left to right ventricle. As a result, the heart has to pump extra blood. It also causes the left side of the heart to become enlarged. |
What causes a ventricular septal defect?
A VSD is a congenital heart defect. This means it’s a problem with the heart’s structure that your child was born with. It can be the only defect, or it can be part of a more complex set of defects. The exact cause is unknown, but most cases seem to occur by chance. Having a family history of heart defects can be a risk factor.
Why is a ventricular septal defect a problem?
Blood normally flows from chamber to chamber in 1 direction through the left and right sides of the heart. With a VSD, blood flows through the defect from the left ventricle to the right ventricle. This is called a left-to-right shunt. It causes more blood than normal to pass through the right side of the heart and lungs. It causes the left side of the heart to become dilated, or enlarged. More blood than normal has to be pumped to the lungs. With a large VSD, the lungs can become filled with extra blood and fluid. When this happens, your child develops a condition called congestive heart failure (CHF). In the case of a large VSD, the extra blood flow can increase the pressure in the pulmonary arteries (blood vessels leading from the heart to the lungs). Over time, this can cause further lung problems.
What are the symptoms?
A child with a small or medium-sized VSD can appear to be in normal health and have no symptoms. A child with a large VSD can develop CHF and will have symptoms. These can include:
Tiredness
Trouble breathing or rapid breathing
Trouble feeding (in infants)
Poor weight gain and growth (in infants)
Fast heart rate
Enlarged liver
Pale skin color
How is a ventricular septal defect diagnosed?
During a physical exam, the doctor checks for signs of a heart problem such as a heart murmur. This is an extra noise caused when blood doesn’t flow smoothly through the heart. If a heart problem is suspected, your child will be referred to a pediatric cardiologist. This is a doctor who diagnoses and treats heart problems in children. To check for a VSD, the following tests may be done:
Chest X-ray. X-rays are used to take a picture of the heart and lungs.
Electrocardiogram (ECG or EKG). The electrical activity of the heart is recorded.
Echocardiogram (echo). Sound waves (ultrasound) are used to create a picture of the heart and look for structural defects.
How is a ventricular septal defect treated?
If your child has CHF symptoms, medications will be prescribed, typically a diurectic or "water pill." They can help reduce the amount of extra fluid in the lungs and ease the work of the heart.
Some VSDs may close on their own. So the cardiologist may check your child’s heart regularly and wait to see if a VSD closes.
If a VSD is large, causes significant symptoms, or doesn’t close on its own, repair is needed. VSD repair is usually done with heart surgery.
Your child’s experience: heart surgery
Heart surgery to repair a VSD is performed by a pediatric heart surgeon. The surgery lasts about 2 to 4 hours. It takes place in an operating room in a hospital. You’ll stay in the waiting room during your child’s surgery.
Before surgery. You’ll be told to keep your child from eating or drinking anything for a certain amount of time before surgery. Follow these instructions carefully.
During surgery. Your child is given medications (sedative and anesthesia) to sleep and not feel pain during surgery. A breathing tube is placed in your child’s trachea (windpipe). Special equipment monitors your child’s heart rate, blood pressure, and oxygen levels. Your child is also placed on a heart-lung bypass machine. This allows blood to continue flowing to the body while the heart is stopped so that it can be operated on. An incision is made in the chest through the sternum (breastbone) to access the heart. The VSD is repaired with stitches or a patch (or both). Then your child is taken off the bypass machine and the chest is closed.
After surgery. Your child is taken to a critical care unit to be cared for and monitored. You can stay with your child during much of this time. He or she may remain in the hospital for 3 to 7 days. When your child is ready to leave the hospital, you’ll be given instructions for home care and follow-up.
Risks and complications of heart surgery
Risks and complications may include:
Reaction to sedative or anesthesia
Incomplete closure of the VSD, requiring further treatment
Arrhythmia (abnormal heart rhythm)
Infection
Bleeding
Nervous system problems, such as seizure or stroke
Abnormal buildup of fluid around the heart and lungs
When to call your healthcare provider
After heart surgery, call the healthcare provider right away if your child has:
Increased pain, swelling, redness, bleeding, or drainage at the incision site
A fever. Talk with your child's doctor to find out at what temperature you should be concerned.
Chest pain
Increased tiredness
Trouble breathing
Nausea or vomiting that contines
A cough that won’t go away
An irregular heartbeat
Passing out
What are the long-term concerns?
A VSD that’s left untreated can lead to further health problems later in life. Your child is more likely to have growth problems, frequent respiratory infections, and develop disease of the blood vessels in the lungs after a year of age.
After treatment, most children with a VSD can be active like other children.
Regular follow-up visits with the cardiologist are needed. The frequency of these visits will likely decrease as your child grows older.
Your child may need to take antibiotics before having any surgery or dental work for 6 months or longer after surgery. This is to prevent infection of the inside lining of the heart and valves. This infection is called infective endocarditis. Discuss this with your child's cardiologist.
Updated:
August 17, 2018
Sources:
Pathophysiology and clinical features of isolated ventricular septal defects in infants and children, Up To Date
Reviewed By:
Ayden, Scott, MD,Bass, Pat F. III, MD, MPH,Image reviewed by StayWell medical illustration team.