Angelman syndrome
Angelman syndrome
Natural Standard Monograph, Copyright © 2013 (www.naturalstandard.com). Commercial distribution prohibited. This monograph is intended for informational purposes only, and should not be interpreted as specific medical advice. You should consult with a qualified healthcare provider before making decisions about therapies and/or health conditions.
Related Terms
Angelman syndrome, chromosome 15q, DNA methylation, genetic counseling, happy puppet syndrome, imprinting, OCA2, UBE3A.
Background
Angelman syndrome is a rare inherited genetic disorder that affects the nervous system. Classic characteristics of Angelman syndrome include developmental delays, intellectual disabilities, severely impaired speech, seizures, a small head, and movement and balance problems. People with Angelman syndrome are typically happy and excitable, may frequently smile and laugh, and may flap their hands often. Other symptoms may include short attention span and fair skin and hair.
The disorder was first described by Dr. Harry Angelman in 1965 when he observed three patients with severe intellectual disabilities, flat heads, jerky body movements, tongues that stuck out, and spontaneous bursts of laughter. Based on these symptoms, the syndrome was known early on as "happy puppet syndrome."
Angelman syndrome is caused by mutations or defects in the UBE3A gene on chromosome 15. The UBE3A gene provides instructions for making the enzyme ubiquitin protein ligase E3A. This enzyme is involved in targeting proteins to be degraded, or broken down, within cells. For example, the p53 protein, which controls cell growth and division, is one of the targets of ubiquitin protein ligase E3A. Protein degradation is a normal process that removes damaged or unnecessary proteins and helps maintain the normal functions of cells. A loss of UBE3A gene function likely causes many of the characteristic features of Angelman syndrome.
Changes in the OCA2 gene are also related to Angelman syndrome. The OCA2 gene provides instructions for making the P protein located in the melanocytes, specialized cells that produce the pigment melanin. Melanin is the substance that gives skin, hair, and eyes their color. Melanin is also found in the light-sensitive tissue of the retina at the back of the eye, where it plays a role in normal vision. Some people with Angelman syndrome have unusually light-colored hair and fair skin, which is thought to be caused by the loss of one copy of the OCA2 gene in each cell. This gene is located in a region of chromosome 15 that is often deleted in individuals with Angelman syndrome.
Most cases of Angelman syndrome are not inherited, or passed down among family members, although there is no indication that individuals with this syndrome are unable to have children. Rather, Angelman syndrome is usually caused by deletion or inactivation of genes on the maternally inherited chromosome 15 in the developing embryo. A healthy person receives two copies of chromosome 15, one from the mother and one from the father. However, in the region of the critical chromosome, the maternal and paternal contribution express certain genes very differently. In a normal individual, the maternal allele (one of two or more versions of a gene) is expressed and the paternal allele is silenced. If the maternal contribution is lost or mutated, the result is Angelman syndrome. Therefore, people affected by this disorder usually have no family history of Angelman syndrome.
The incidence of Angelman syndrome is estimated to be about one in 12,000-20,000 people. Limited data suggest that people with Angelman syndrome have nearly-normal life spans.
Risk Factors
Because Angelman syndrome is caused by a spontaneous mutation or defect in the egg or sperm cells or the developing embryo, no risk factors have been identified. In rare cases, the disorder is inherited, or passed down among family members. In these cases, a family history of Angelman syndrome is a risk factor for the disorder. The incidence of Angelman syndrome is estimated to be about one in 12,000-20,000 people.
Causes
About 70% of Angelman syndrome cases occur as the result of a spontaneous genetic mutation or defect in the egg or sperm cells or in the developing embryo. The remaining cases of Angelman syndrome may be inherited, or passed down among family members.
Individuals usually inherit two copies of the UBE3A gene, one from each parent. This gene functions in many parts of the body. In the brain, however, only the copy inherited from the mother is active. If the gene copy from the mother is damaged or lost because of a genetic mutation, the individual will have no active copy of the gene in his or her brain. This unequal expression of genes from the mother and father is known as imprinting.
About 85% of Angelman syndrome cases are caused by a mutation or defect in the UBE3A gene, which provides instructions for making the enzyme ubiquitin-protein ligase E3A, which is involved in targeting proteins to be degraded, or broken down, within cells. This defect may be responsible for the intellectual disabilities and memory deficits observed in individuals with Angelman syndrome. The causes of the remainder of cases are currently unknown. There are four known means by which a mutation in the UBE3A gene occurs. Of the 85% of Angelman syndrome cases in which UBE3A is defective, about 70% are caused by a missing piece of chromosome 15, resulting in at least a partial deletion of the gene. In about 11% of cases, the syndrome is caused by a defect in the copy of the gene inherited from the mother. In a small percentage of Angelman syndrome cases, an individual inherits two copies of the UBE3A gene from the father, rather than one from the father and one from the mother, making the gene completely inactive. This is called paternal uniparental disomy. In even fewer cases, the region of deoxyribonucleic acid (DNA) that controls the UBE3A gene is rearranged in what is called a translocation, which occurs when genetic material is rearranged between two noncorresponding chromosomes.
The OCA2 gene, which is also located on chromosome 15, is sometimes deleted in Angelman syndrome, because it is located close to the UBE3A gene. The OCA2 gene provides instructions for making the P protein. This protein is located in the melanocytes, specialized cells that produce the pigment melanin, which gives skin, hair, and eyes their color. Melanin is also found in the light-sensitive tissue of the retina at the back of the eye, where it plays a role in normal vision. Some people with Angelman syndrome have unusually light-colored hair and fair skin, which is thought to be caused by a loss of one copy of the OCA2 gene in each cell. This gene is located in a region of chromosome 15 that is often deleted in individuals with Angelman syndrome. A small percentage of people with Angelman syndrome also have oculocutaneous albinism type 2. In addition to a deletion in one copy of chromosome 15, these people also have a mutation in the OCA2 gene on the other copy of chromosome 15.
Signs and Symptoms
General: At birth, people with Angelman syndrome appear to be normally developed, as evidenced by a normal birthweight and head circumference. They may have feeding difficulties during infancy as a result of a decreased sucking reflex. While developmental delays may become apparent at about six months of age, the typical symptoms of Angelman syndrome described below are usually not apparent until after one year of age.
Cognitive development: People with Angelman syndrome tend to have severe developmental delays in motor, social, language, or thinking skills. They also tend to have intellectual disabilities. Short attention span, hyperactivity, and sleep problems are common in patients with Angelman syndrome. People with Angelman syndrome may have a happy and excitable demeanor, and they may frequently smile and laugh. Speech impairment is profound. People with Angelman syndrome can rarely use even two words consistently.
Face and head: A small head is a common symptom of Angelman syndrome that may be apparent by one year of age. In some individuals, the back of the head is flat, the tongue sticks out, the mouth is wide, and the teeth are widely spaced.
Nervous system: Angelman syndrome is a neurogenetic disorder, and about 10% of affected individuals never learn to walk. Those who do typically begin to walk between the ages of two and a half and six. People with Angelman syndrome may have an unsteady gait, poor coordination and balance, arms and legs that tremble or shake, and a flapping motion of the hands and forearms. In addition, many people with Angelman syndrome have seizures, which tend to begin between ages one and three.
Speech problems: People with Angelman syndrome have profound speech impairment. It is rare for an individual with this syndrome to reliably use even two words. These patients tend not to respond to instruction in sign language and instead communicate by other means, such as pointing.
Other: Other symptoms that may be seen in patients with Angelman syndrome include fair-colored skin and eyes, constipation, obesity, scoliosis (sideways curvature of the spine), strabismus (crossed eyes), a wide mouth with widely spaced teeth, drooling, gastroesophageal reflux, sensitivity to heat, and a fascination with water and "crinkly" items such as paper or foil. People with Angelman syndrome may have sleep disturbances, including an abnormal sleep-wake cycle, frequent waking at night, and awakening early.
Diagnosis
General: At birth, people with Angelman syndrome appear to be normally developed, with normal weight and head circumference. There also may be feeding difficulties. While developmental delays may become apparent at about six months of age, the typical symptoms of Angelman syndrome are usually not apparent until after one year of age. Angelman syndrome may first be suspected when a toddler does not achieve normal developmental milestones, such as the attainment of gross motor skills and development of early speech skills.
Patients with Angelman syndrome tend to have a happy and excitable demeanor, with frequent bursts of laughter and hyperactivity. While about 10% of patients with Angelman syndrome never learn to walk, others begin walking between the ages of two and a half and six. The gait tends to be unstable and may appear jerky and robot-like. In addition, the arms and legs may tremble and the hands and forearms may make flapping motions.
Puberty tends to be normal, and fertility does not appear to be affected. Young adults with Angelman syndrome appear to be in generally good health unless they have seizures.
Physical exam: During a physical exam, a doctor will note decreased muscle tone and increased reflexes. In addition, patients may smile, laugh, or lean toward a vibrating tuning fork emitting sound.
Eye exam: A thorough eye exam may reveal an eye problem known as strabismus, in which one or both of the eyes turn in, out, up, or down. Although strabismus has been associated with Angelman syndrome, it does not affect all patients with this syndrome and thus may not be a diagnostic symptom.
Electroencephalogram (EEG): An electroencephalogram can measure electrical activity in the brain using electrodes placed on a person's scalp. At one end are action potentials in a single axon of a nerve cell in the brain, and at the other activity measured by the EEG, which aggregates the electric voltage fields from millions of neurons. The EEG is collected from tens to hundreds of electrodes positioned on different locations on the surface of the head. An EEG in a person with Angelman syndrome may show abnormal electrical activity, especially during seizures.
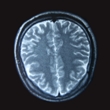
Brain magnetic resonance imaging (MRI): Magnetic resonance imaging (MRI) is used to visualize soft tissues in the body. It uses a powerful magnetic field to align hydrogen atoms in water in the body. An MRI of the brain may show some breakdown of brain tissue and deterioration of the lining of the nerve cells, although individuals with Angelman syndrome typically do not show any brain abnormalities except for mild cortical atrophy or demyelination of neurons. Myelin is a sheathlike membrane that covers neurons and helps transmit electrical messages from neuron to neuron. If this myelin sheath is broken down, it can lead to a slight decrease in brain function.
Speech testing: All individuals with Angelman syndrome will display a speech impairment, characterized by no or minimal use of words. Receptive and nonverbal communication skills are more developed than verbal communication skills.
Genetic testing: Only about 85% of Angelman syndrome cases can be confirmed by genetic testing, because only this percentage of affected individuals have a defect in the gene that causes Angelman syndrome. If Angelman syndrome is suspected, a deoxyribonucleic acid (DNA) test may be performed to confirm a diagnosis. A sample of the patient's blood is taken and analyzed in a laboratory for the defect in the UBE3A gene. If this defect is detected, a positive diagnosis is made.
Prenatal DNA testing: Prenatal testing may be performed to determine whether the fetus has Angelman syndrome. Amniocentesis and chorionic villus sampling (CVS) can diagnose this disorder. However, because there are serious risks associated with these tests, patients should discuss the potential health benefits and risks with a medical professional.
During amniocentesis, a long, thin needle is inserted through the abdominal wall and into the uterus, and a small amount of amniotic fluid is removed from the sac surrounding the fetus. Cells in the fluid are then analyzed for normal and abnormal chromosomes. This test is performed after 15 weeks of pregnancy. The risk of miscarriage is about one in 200-400 patients. Some patients may experience minor complications, such as cramping, leaking fluid, or irritation where the needle was inserted.
During chorionic villus sampling (CVS), a small piece of tissue (chorionic villi) is removed from the placenta between the ninth and 14th weeks of pregnancy. CVS may be performed through the cervix or through the abdomen. The cells in the tissue sample are then analyzed for the mutation in the UBE3A gene. Miscarriage occurs in about 0.5-1% of women who undergo this procedure.
Complications
Constipation: Some individuals with Angelman syndrome may have chronic constipation.
Limited mobility: Depending on individual characteristics related to developmental delays and muscle strength, patients with Angelman syndrome may have mild-to-severe limitation of mobility, including fine tremors, jerky limb movements, hand flapping, and a wide-based, stiff-legged gait.
Seizures: Seizures are a common problem in Angelman syndrome. Seizures may be rare or recurrent, mild or severe, and worsened by other factors such as fever. Seizure activity may lessen with age in some individuals with Angelman syndrome. Seizures may have serious consequences. Intense, rapid muscle contractions can cause injuries, including broken bones. Sudden loss of consciousness can cause serious injury from falls and accidents. People may have numerous seizures without incurring serious brain damage. However, seizures that recur and cause convulsions may eventually impair intelligence.
Treatment
General: There is no cure for Angelman syndrome. Instead, treatment aims to reduce symptoms and prevent complications. People with Angelman syndrome should also be examined regularly by a geneticist, neurologist (nerve specialist), ophthalmologist (eye specialist), and a gastroenterologist.
Anticonvulsant drugs: Individuals with severe seizures may require anticonvulsant drugs. Valproic acid (Depakene®, Depakote®), clonazepam (Klonopin®), topiramate (Topamax®), and lamotrigine (Lamictal®) may be used in patients with Angelman syndrome, while vigabatrin (Sabril®) and tiagabine (Gabitril®) should be avoided. Anticonvulsants can completely prevent generalized seizures in about one-third of people who have them and greatly reduce the frequency of seizures in another third. Almost two-thirds of people who respond to anticonvulsants can eventually stop taking them without having a relapse. However, anticonvulsants are ineffective in about 10-20% of people with a seizure disorder. Anticonvulsants may have side effects. Many cause drowsiness, but some may make children hyperactive. Blood tests are done periodically to determine whether an anticonvulsant is impairing kidney or liver function or reducing the number of blood cells.
Assisted-mobility devices: Some people may require assisted-mobility devices to help them walk. These devices may include a cane, a walker, braces, a wheelchair, or a mobilized chair. Individuals should talk with a healthcare provider to determine their best options. Adaptive equipment, such as a wheelchair, may also be needed for very young children with hyperactivity to decrease the risk of injury.
Behavioral therapy: Behavioral therapy may also be beneficial. Several different types of behavioral therapy may help patients with Angelman syndrome improve their communication and social skills, as well as learning abilities and adaptive behaviors. Therapy may also help reduce negative behaviors, such as inappropriate laughter and hyperactivity. For instance, dialectical behavior therapy (DBT), a psychologically based method, may be used to teach behavioral skills to help a person tolerate stress, regulate emotions, and improve relationships with others. Key elements that DBT practitioners emphasize include behaviorist theory, dialectics, cognitive therapy, and DBT's central component, mindfulness. Evidence suggests that behavioral therapy is most effective when it is started early in life.
Dental care: Patients with Angelman syndrome should receive good preventive dental care, including regular flossing, teeth brushing, and visits to the dentist.
Education: By law, individuals with Angelman syndrome must have access to education that is tailored to their needs. According to the Individuals with Disabilities Education Act, all children with disabilities in the United States must receive free and appropriate education from age three until the end of high school or until they are 21 years old, whichever occurs first.
If a child has intellectual disabilities, staff members of the patient's school should consult with the patient's parents or caregivers to design an individualized education plan. The school faculty must document the child's progress in order to ensure that the child's needs are being met.
Educational programs vary among patients depending on the severity of the person's intellectual and learning disabilities. In general, most experts believe that children with disabilities should be educated alongside their nondisabled peers. It is believed that nondisabled students will help the patient learn appropriate behavioral, social, and language skills. Depending on their needs, patients with intellectual disabilities may be educated in mainstream classrooms, attend public schools but take special education classes, or attend specialized schools that are equipped to teach children with disabilities.
Feeding difficulties: Infants with Angelman syndrome who have feeding difficulties may require special nipples, drugs to treat reflux, and tube feeding.
Ketogenic diet: A ketogenic diet is a high-fat, adequate-protein, low-carbohydrate diet used to treat some forms of epilepsy in children. The diet mimics aspects of starvation by forcing the body to burn fat rather than carbohydrate stores. Normally, the carbohydrates in food are converted into glucose, which is then transported around the body and is particularly important in fueling the brain. However, if there is very little carbohydrate in the diet, the liver converts fat into fatty acids and ketone bodies. The ketone bodies pass into the brain and replace glucose as an energy source. When the body produces ketone bodies (a state known as ketosis), an anticonvulsive effect occurs. This diet may help individuals with severe seizures that are inadequately controlled by drugs.
Laxatives: Patients who have constipation may benefit from a high-fiber diet as well as laxative medications such as stool softeners.
Occupational therapy: Patients with moderate-to-severe intellectual disabilities may benefit from occupational therapy. During sessions, a therapist helps the child learn skills to help him or her perform basic daily tasks, such as feeding, dressing, and communicating with others. There are therapists who specialize in patients with specific disorders. Parents and caregivers can ask their child's pediatrician to recommend therapists.
Physical therapy: Physical therapy may help patients with Angelman syndrome improve their physical strength and motor coordination. A variety of techniques, including exercises, stretches, traction, electrical stimulation, and massage are used during physical therapy sessions. A therapist may also teach parents or caregivers how to exercise a baby's muscles.
Speech-language therapy: Individuals with Angelman syndrome may benefit from speech-language therapy. During speech-language therapy, a qualified speech-language professional (SLP) works with the patient on a one-to-one basis, in a small group, or in a classroom to overcome speech and language problems. Programs are tailored to the patient's individual needs. On average, patients receive five or more hours of therapy per week for three months to several years. Speech pathologists use a variety of exercises to improve the patient's communication skills, with a focus on nonverbal communication for patients with Angelman syndrome.
Sedative drugs: Patients with sleeping problems may benefit from the use of sedative drugs such as chloral hydrate (Aquachloral®, Noctec®), which is safe when taken exactly as prescribed. There is a risk of overdose with chloral hydrate, as with all sedatives. Side effects include headache, stomach upset, dizziness, and an unpleasant taste in the mouth. Diphenhydramine (Benadryl®) is also used. Side effects of this medication include headache and dizziness.
Stimulant drugs: Some children with Angelman syndrome may benefit from the use of stimulant drugs such as methylphenidate (Concerta®, Metadate®, Methylin®, Ritalin®) to control hyperactivity. Stimulant drugs should not be used in children under six years of age, because their safety and efficacy have not been established in this age group. Although a causal relationship has not been established, suppression of growth has been reported with long-term use of stimulants in children. Nervousness and insomnia are the most common side effects. Others include nausea, dizziness, heart palpitations, headache, increased or decreased blood pressure, and abdominal pain.
Support groups: There are several support groups that offer individuals with Angelman syndrome and their families a community, education resources, and emotional support.
Surgery: If strabismus (crossed eyes) is severe, it may require surgical correction. In addition, surgery may be needed to correct orthopedic problems that cause pain or limit mobility. Scoliosis (sideways curvature of the spine) may be corrected by a surgical procedure called "rodding," in which a rod is surgically inserted to help correct and stabilize spinal position.
Other: Families of an Angelman syndrome child may choose to build a "safe" environment, in which characteristic behaviors cannot lead to self injury. This may include removal of hard surfaces and sharp corners.
Experimental therapies: There are ongoing scientific studies of high-dose oral folate and betaine for the treatment of Angelman syndrome. In theory, these treatments may increase brain activity of the paternal form of the UBE3A gene. However, the safety and effectiveness of these treatments have not yet been established.
Integrative Therapies
Currently there is a lack of scientific evidence on the use of integrative therapies for the treatment or prevention of Angelman syndrome.
Prevention
Because most cases of Angelman syndrome are caused by spontaneous genetic mutations, there is currently no known way to prevent the disease.
Genetic counseling to assess risks to siblings and other family members is based on knowing the mechanism involved in causing the loss of expression of this genetic region at the molecular level. Recurrence risks to parents and extended family members vary from a negligible risk of recurrence to a possible 50% risk.
Author Information
This information has been edited and peer-reviewed by contributors to the Natural Standard Research Collaboration (www.naturalstandard.com).
Bibliography
Natural Standard developed the above evidence-based information based on a thorough systematic review of the available scientific articles. For comprehensive information about alternative and complementary therapies on the professional level, go to www.naturalstandard.com. Selected references are listed below.
American Epilepsy Society www.aesnet.org.
American Society of Human Genetics/American College of Medical Genetics Test and Technology Transfer Committee. Diagnostic testing for Prader-Willi and Angelman syndromes. Am J Hum Genet. 1996;58: 1085-8. View Abstract
Angelman Syndrome Foundation. www.angelman.org.
Buiting K, Dittrich B, Gross S, et al. Sporadic imprinting defects in Prader-Willi syndrome and Angelman syndrome: implications for imprint-switch models, genetic counseling, and prenatal diagnosis. Am J Hum Genet. 1998;63: 170-80. View Abstract
Buntinx IM, Hennekam RCM, Brouwer OF, et al. Clinical profile of Angelman syndrome at different ages. Am J Med Genet. 1995;56: 176-83. View Abstract
Epilepsy Foundation www.efa.org.
Magenis RE, Moncla A, Schinzel AA, et al. Angelman syndrome 2005: updated consensus for diagnostic criteria. Am J Med Genet. 2006;140A: 413-8. View Abstract
Natural Standard: The Authority on Integrative Medicine. www.naturalstandard.com.
Stalker HJ, Williams CA. Genetic counseling in Angelman syndrome: the challenges of multiple causes. Am J Med Genet. 1998;77: 54-9, 1998. View Abstract
Copyright © 2013 Natural Standard (www.naturalstandard.com)
The information in this monograph is intended for informational purposes only, and is meant to help users better understand health concerns. Information is based on review of scientific research data, historical practice patterns, and clinical experience. This information should not be interpreted as specific medical advice. Users should consult with a qualified healthcare provider for specific questions regarding therapies, diagnosis and/or health conditions, prior to making therapeutic decisions.
Updated:
March 22, 2017